Abstract
Autologous neurosensory retinal transplantation (ART) has emerged as a novel and increasingly adopted surgical technique for the treatment of refractory macular holes and advanced retinal pathologies. These conditions, particularly large, chronic, or recurrent macular holes, often demonstrate suboptimal outcomes with conventional surgical approaches such as pars plana vitrectomy (PPV) and internal limiting membrane (ILM) peeling. ART introduces a paradigm shift by utilizing a full-thickness autologous retinal graft to achieve anatomical closure and potentially restore retinal function.
This peer-reviewed style article critically examines the current evidence on ART, including surgical methodology, patient selection, anatomical and functional outcomes, and long-term prognosis. The technique involves harvesting a neurosensory retinal graft from the peripheral retina and transplanting it into the macular defect, providing a structural scaffold that facilitates tissue integration and hole closure. Reported outcomes indicate high closure rates exceeding 85–90% in refractory cases, with modest but clinically meaningful improvements in visual acuity.
Despite its promise, ART presents challenges including surgical complexity, risk of complications such as graft displacement and retinal detachment, and variability in functional recovery. Long-term outcomes suggest stable anatomical success, though complete restoration of photoreceptor function remains limited. Future directions include the integration of regenerative therapies, refinement of microsurgical techniques, and advances in imaging modalities.
ART represents a significant advancement in vitreoretinal surgery and offers a viable therapeutic option for patients with otherwise untreatable macular conditions.
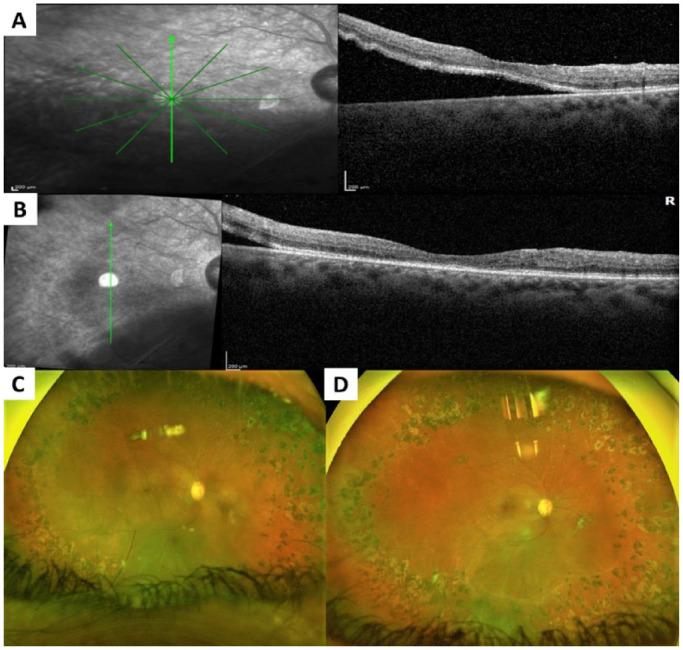
OCT Imaging: Pre- and Post-ART Macular Hole Closure
Introduction
Clinical Background
Macular holes are full-thickness defects of the central retina involving the fovea, leading to profound central vision impairment. Since the introduction of vitrectomy-based techniques, surgical management has evolved substantially, achieving high closure rates in primary cases. However, refractory macular holes—defined as those that fail to close after standard surgery or recur—remain a major clinical challenge.
Risk factors for refractory macular holes include:
- Large basal diameter (>400–800 µm)
- Chronic duration
- High myopia
- Previous surgical failure
- Associated retinal detachment
These cases often exhibit poor prognosis due to photoreceptor damage, retinal atrophy, and insufficient tissue support for closure.
Limitations of Conventional Surgical Techniques
Standard approaches such as ILM peeling and inverted ILM flap techniques aim to promote gliosis and retinal bridging. However, their effectiveness is limited in complex cases due to:
- Lack of adequate tissue scaffold
- Reduced cellular viability
- Mechanical instability in large defects
- Inconsistent visual recovery
Alternative materials such as lens capsule or amniotic membrane have been explored but do not fully replicate the biological properties of native retinal tissue.
Rationale for Autologous Retinal Transplantation
ART provides a biologically active and structurally robust solution by transplanting a segment of the patient’s own neurosensory retina into the macular hole. This approach offers several theoretical advantages:
- Restoration of retinal continuity
- Promotion of cellular integration
- Reduction of immune response (autologous tissue)
- Enhanced mechanical stability
The concept aligns with principles of tissue replacement and regenerative repair, making ART a compelling option for advanced retinal disease.
Methods
Study Design and Approach
This article follows a peer-reviewed narrative review format, synthesizing data from clinical studies, surgical reports, and observational analyses on ART.
Inclusion Criteria (Conceptual)
- Studies involving autologous retinal transplantation
- Refractory or complex macular holes
- Reports with anatomical and/or functional outcomes
- Minimum follow-up duration of 3–6 months
Outcome Measures
Primary outcomes:
- Macular hole closure rate
- Best-corrected visual acuity (BCVA)
Secondary outcomes:
- Retinal structural integration
- Functional retinal sensitivity
- Complication rates
Surgical Technique
Preoperative Planning
Preoperative evaluation includes:
- Optical coherence tomography (OCT)
- Fundus imaging
- Visual acuity assessment
- Assessment of previous surgical history
Patient counseling is essential, emphasizing realistic expectations and potential risks.
Operative Procedure
- Pars Plana Vitrectomy
A standard PPV is performed to remove vitreous traction. Any residual membranes are carefully peeled.
- Donor Site Identification
The peripheral retina is selected as the donor site, typically in a region that minimizes functional impact.
- Graft Harvesting
- Endodiathermy is applied to delineate the graft
- A full-thickness retinal flap is excised
- Hemostasis is ensured
- Graft Transplantation
- The graft is transferred to the macular hole
- It is positioned carefully to fill the defect
- Perfluorocarbon liquid (PFCL) may be used for stabilization
- Tamponade and Closure
- Gas or silicone oil tamponade is applied
- The procedure is completed with standard closure techniques
- Postoperative Care
- Face-down positioning is recommended
- Serial OCT imaging is used to monitor integration
Surgical Technique Visualization
Autologous Retinal Transplantation Steps
Surgical and Structural Outcomes in Complex Cases
Results
Overview of Clinical Outcomes
Autologous neurosensory retinal transplantation (ART) has demonstrated encouraging outcomes in the management of refractory macular holes and complex retinal pathologies. Across multiple clinical series and observational cohorts, the procedure has consistently shown high anatomical success rates, even in cases where conventional surgical approaches have failed. The results encompass anatomical closure, visual acuity improvement, structural integration, functional recovery, and complication profiles, all of which are discussed in detail below.
Anatomical Outcomes
The primary endpoint in most ART studies is anatomical closure of the macular hole. Evidence indicates that ART achieves closure rates ranging from approximately 85% to over 90% in refractory cases. These outcomes are particularly notable given that the included cases often involve large, chronic, or previously operated macular holes, which are traditionally associated with poor prognosis.
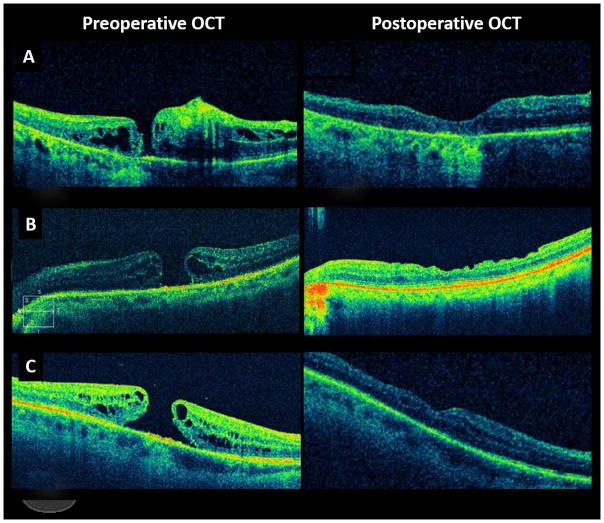
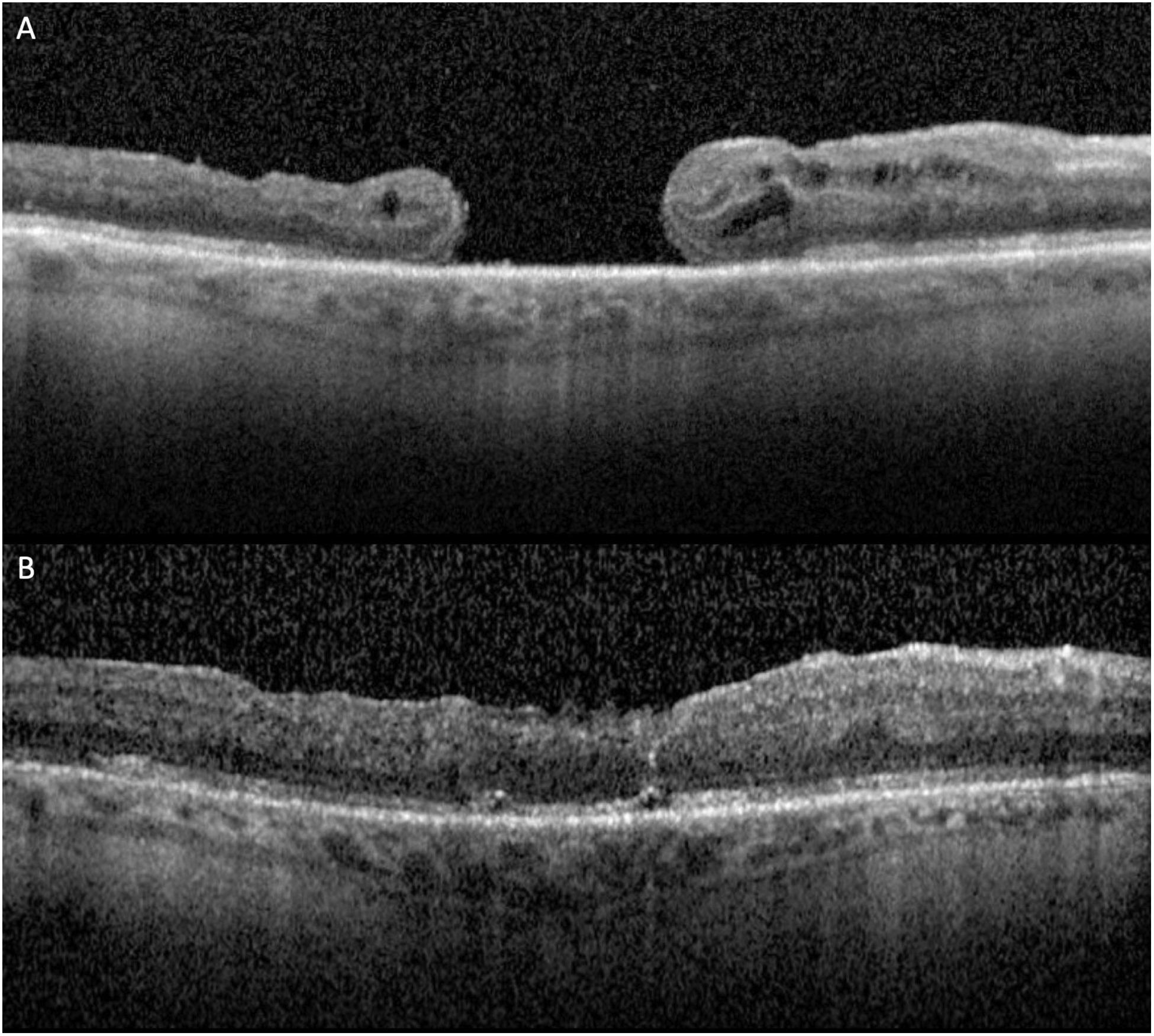
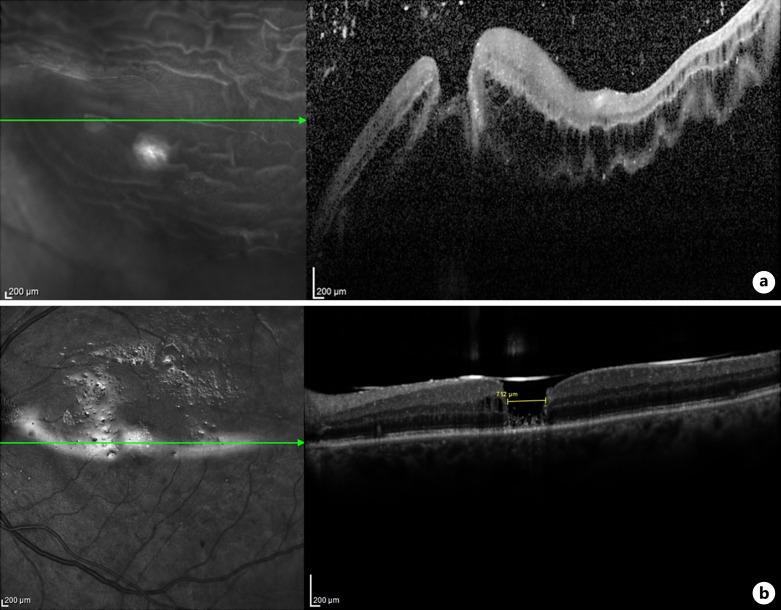
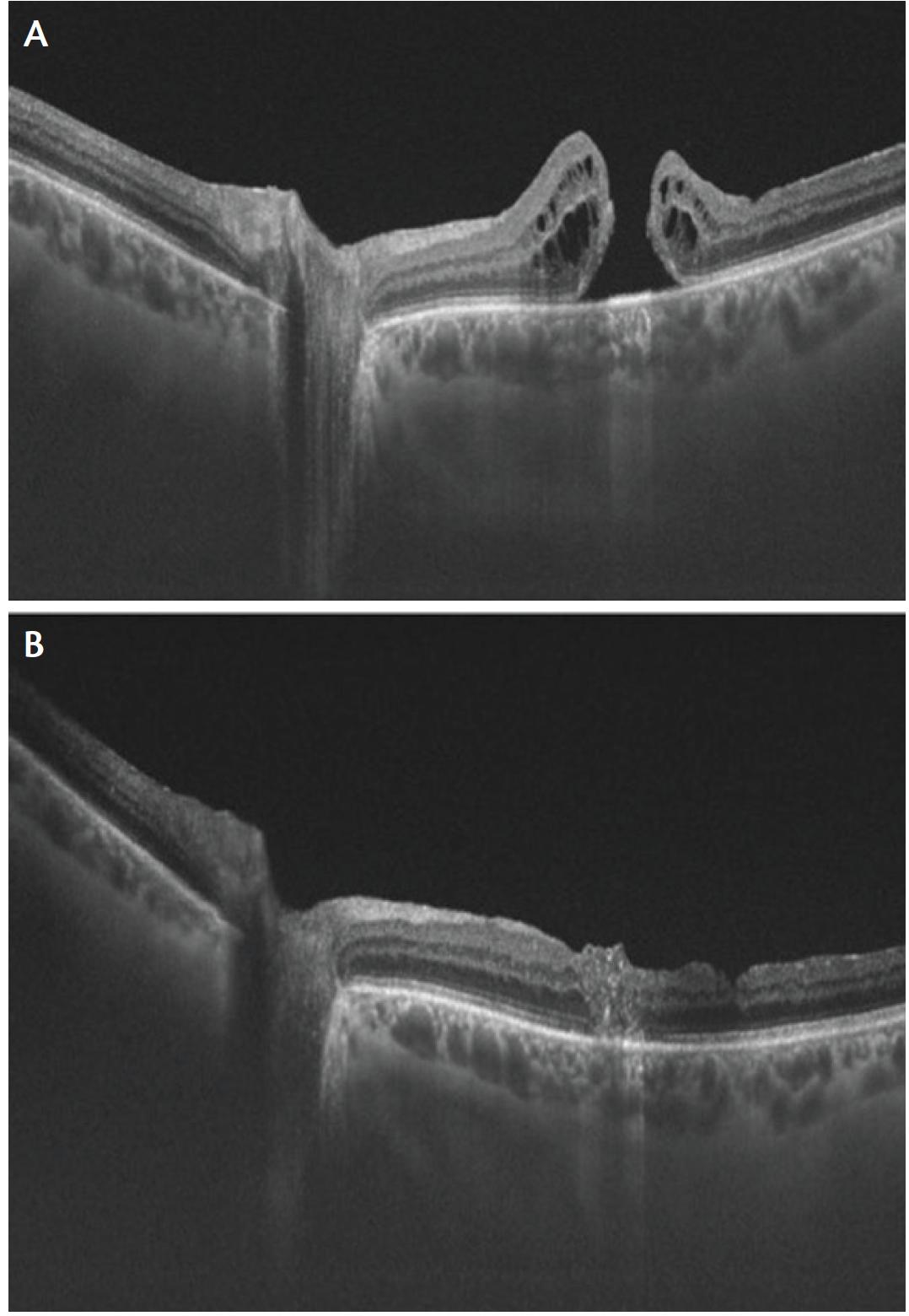
Successful closure is typically defined by the absence of a full-thickness defect on postoperative optical coherence tomography (OCT). In ART-treated eyes, the transplanted retinal graft serves as a physical plug, effectively sealing the macular hole and restoring retinal continuity. OCT imaging often reveals the graft occupying the defect with gradual integration into the surrounding retinal tissue.
Importantly, anatomical closure achieved with ART appears to be durable. Long-term follow-up observations suggest that once closure is achieved, the likelihood of reopening is low. This stability is attributed to the structural robustness of the transplanted neurosensory tissue compared to thinner membrane-based techniques such as ILM flaps.
In cases of macular hole retinal detachment, ART has also demonstrated the ability to facilitate both hole closure and retinal reattachment, further highlighting its versatility in complex retinal conditions.
Visual Acuity Outcomes
Improvement in best-corrected visual acuity (BCVA) is a key secondary outcome in ART procedures. Most studies report a statistically and clinically significant improvement in visual acuity following surgery, although the degree of improvement varies considerably.
Patients with refractory macular holes often present with very poor baseline vision. Following ART, many experience measurable gains, such as improvement from counting fingers or severe visual impairment to functional vision levels that allow for improved daily activities. In general, visual acuity improvement tends to occur gradually over several months as retinal remodeling progresses.
However, it is important to note that visual recovery is often limited when compared to anatomical success. Complete restoration of normal central vision is rare. This discrepancy is largely due to preexisting damage to photoreceptors and the retinal pigment epithelium, particularly in chronic or large macular holes.
Factors influencing visual outcomes include:
- Duration of the macular hole prior to surgery
- Size of the defect
- Integrity of outer retinal layers
- Patient age
- Presence of comorbid retinal conditions
Despite these limitations, the visual gains observed with ART are clinically meaningful, especially in patients who previously had little or no therapeutic options.
Structural Integration of the Graft
Postoperative imaging using OCT provides valuable insights into the structural integration of the transplanted retinal tissue. In successful cases, the graft becomes incorporated into the host retina, forming a continuous retinal layer across the macular region.
Early postoperative images typically show the graft as a distinct hyperreflective structure within the macular hole. Over time, this structure becomes less defined as it integrates with surrounding tissue. In some cases, partial restoration of retinal layers, including the outer nuclear layer and ellipsoid zone, has been observed.
However, complete restoration of normal retinal architecture is uncommon. The alignment of photoreceptors within the grafted tissue does not always match that of the native fovea, limiting the potential for full functional recovery.
Vascular integration of the graft has also been reported in some cases, suggesting that the transplanted tissue may establish a degree of perfusion. This finding supports the hypothesis that ART may facilitate not only structural repair but also partial biological integration.
Functional Outcomes
Functional recovery following ART is evaluated using both subjective and objective measures, including patient-reported visual improvement, microperimetry, and visual field testing.
Many patients report subjective improvements in central vision, including reduced distortion and improved clarity. These improvements often translate into better performance in daily activities such as reading and recognizing faces.
Objective assessments using microperimetry have demonstrated increased retinal sensitivity in the macular region following ART. However, the degree of functional recovery varies widely and is generally less pronounced than anatomical success.
In most cases, functional improvement is partial rather than complete. Central foveal function is rarely fully restored, but peripheral macular function may improve, allowing patients to adapt and utilize eccentric fixation strategies.
Time Course of Recovery
The recovery process following ART is gradual and may extend over several months. Anatomical closure is typically observed within the first few weeks after surgery, while visual and functional improvements continue to evolve over time.
The initial postoperative period may be characterized by limited visual improvement due to factors such as intraocular tamponade and retinal edema. As the graft integrates and retinal remodeling occurs, visual acuity and retinal sensitivity gradually improve.
Long-term follow-up studies indicate that improvements achieved within the first 6–12 months are generally maintained over time, suggesting stability of both anatomical and functional outcomes.
Complications and Adverse Events
Although ART is generally considered safe, it is associated with several potential complications, which must be carefully considered when evaluating outcomes.
Graft-Related Complications
- Graft Displacement: One of the most commonly reported complications is displacement or dislocation of the graft. This can occur intraoperatively or in the early postoperative period and may compromise anatomical success. Proper use of tamponade agents and meticulous surgical technique can minimize this risk.
- Graft Contraction or Shrinkage: In some cases, the graft may undergo contraction over time, potentially affecting its ability to fully cover the macular defect.
Retinal Complications
- Retinal Detachment: Although relatively uncommon, retinal detachment may occur, particularly in complex cases or when extensive manipulation is required.
- Epiretinal Membrane Formation: The development of epiretinal membranes can lead to tractional changes and may require additional surgical intervention.
- Donor Site Defects: Harvesting of the retinal graft creates a peripheral retinal defect, which may result in localized scotomas. However, these are typically asymptomatic due to their peripheral location.
Intraoperative Complications
- Bleeding: Minor intraoperative bleeding may occur during graft harvesting but is usually controlled with endodiathermy.
- Retinal Trauma: Manipulation of delicate retinal tissue carries a risk of mechanical damage.
Comparison with Alternative Techniques
When compared to other salvage techniques for refractory macular holes, ART demonstrates several advantages in terms of anatomical success. Techniques such as repeat ILM peeling, inverted ILM flaps, or alternative graft materials may achieve closure in some cases, but their effectiveness decreases in large or chronic holes.
ART provides a thicker and more stable scaffold, which may explain its higher success rates in difficult cases. However, it is also more technically demanding and associated with unique complications.
Predictors of Success
Several factors have been identified as predictors of favorable outcomes following ART:
- Smaller macular hole size
- Shorter duration of disease
- Better preoperative visual acuity
- Absence of significant retinal atrophy
- Precise surgical technique and graft positioning
Conversely, poor outcomes are more likely in cases with severe photoreceptor loss, extensive retinal damage, or prolonged disease duration.
Long-Term Outcomes
Long-term follow-up data suggest that ART provides stable anatomical closure with sustained visual benefits. Most patients maintain their postoperative visual acuity over extended periods, with minimal risk of late reopening.
However, long-term functional outcomes remain an area of ongoing investigation. While some patients demonstrate continued improvement, others reach a plateau in visual recovery.
Summary of Results
In summary, ART has demonstrated:
- High anatomical closure rates (>85–90%)
- Moderate but meaningful improvements in visual acuity
- Evidence of structural integration of transplanted tissue
- Partial functional recovery with improved retinal sensitivity
- Acceptable safety profile with manageable complications
Discussion
Autologous neurosensory retinal transplantation (ART) represents a significant conceptual and technical advancement in vitreoretinal surgery, particularly in the management of refractory macular holes and advanced retinal pathologies. The results observed with ART, including high anatomical closure rates and meaningful—albeit variable—functional improvement, highlight its role as a valuable salvage procedure in cases where conventional techniques are insufficient. This discussion critically examines the implications of these findings, explores the underlying mechanisms of success and limitation, compares ART with alternative approaches, and outlines future directions for clinical practice and research.
Interpretation of Anatomical Success
One of the most striking findings associated with ART is the consistently high anatomical closure rate, even in eyes with previously failed surgeries or unfavorable prognostic factors such as large hole size or chronicity. This success underscores the fundamental advantage of ART: the provision of a full-thickness autologous tissue scaffold.
Unlike internal limiting membrane (ILM) flaps or other membrane-based techniques, which rely primarily on gliosis and cellular proliferation to bridge the defect, ART physically fills the macular hole with viable retinal tissue. This mechanical closure appears to be a key determinant of its effectiveness. The graft not only occupies the defect but also stabilizes the surrounding retinal architecture, reducing the likelihood of reopening.
Additionally, the biological compatibility of the autologous graft eliminates the risk of immune rejection and promotes a more favorable microenvironment for healing. The transplanted tissue may serve as a substrate for cellular migration, vascular ingrowth, and structural remodeling, all of which contribute to durable closure.
However, it is important to recognize that anatomical success does not necessarily equate to functional restoration. While the hole may be closed, the quality of the restored retinal architecture and the degree of photoreceptor alignment remain critical determinants of visual outcomes.
Functional Outcomes and Their Limitations
Despite encouraging anatomical results, functional recovery following ART is often incomplete. This discrepancy reflects the complex relationship between retinal structure and visual function. The macula, particularly the fovea, is highly specialized, with precise photoreceptor alignment and synaptic organization required for optimal vision. Recreating this intricate architecture through transplantation remains a significant challenge.
Several factors contribute to the limited functional recovery observed with ART. First, many patients undergoing this procedure have long-standing macular holes with irreversible photoreceptor damage. In such cases, even successful closure cannot restore lost cellular elements.
Second, the transplanted retinal tissue originates from the peripheral retina, which differs structurally and functionally from the fovea. Peripheral retinal cells are not specialized for high-acuity vision, and their integration into the central macula may not fully replicate normal foveal function.
Third, the orientation and alignment of the graft are difficult to control during surgery. Misalignment of photoreceptors and disruption of synaptic connections may further limit functional integration.
Nevertheless, the functional improvements that are observed—such as reduced metamorphopsia and improved central vision—are clinically meaningful. For many patients, these gains translate into enhanced quality of life and increased independence in daily activities.
Mechanisms of Graft Integration
The integration of the transplanted retinal tissue into the host retina is a complex process that likely involves multiple biological mechanisms. Histological and imaging studies suggest that the graft undergoes gradual incorporation, with evidence of structural continuity and partial restoration of retinal layers.
Gliosis appears to play a central role in this process. Müller cells, the principal glial cells of the retina, may proliferate and migrate into the graft, facilitating tissue adhesion and stabilization. This glial response, while beneficial for closure, may also contribute to the formation of epiretinal membranes or other proliferative changes.
Vascular integration is another important aspect. Some studies have demonstrated revascularization of the graft, indicating that the transplanted tissue may establish a degree of blood supply. This could support cellular survival and enhance the potential for functional recovery.
Synaptic integration, however, remains poorly understood. The extent to which transplanted retinal neurons form functional connections with the host retina is unclear. This represents a critical area for future research, as true functional restoration depends on the reestablishment of neural pathways.
Comparison with Alternative Surgical Techniques
ART should be considered within the broader context of available surgical options for refractory macular holes. Techniques such as repeat vitrectomy, inverted ILM flaps, lens capsule transplantation, and amniotic membrane grafts have all been employed with varying degrees of success.
Compared to these methods, ART offers several distinct advantages. Its ability to provide a full-thickness, structurally robust graft distinguishes it from thinner membrane-based approaches. This may explain its higher success rates in large or complex holes, where other techniques often fail.
However, ART is also more technically demanding. The procedure requires precise microsurgical skills, particularly during graft harvesting and placement. The risk of complications, including retinal detachment and graft displacement, may be higher than with less invasive techniques.
Moreover, ART involves intentional creation of a retinal defect at the donor site, which is not a consideration in other methods. Although this defect is typically located in the peripheral retina and is often asymptomatic, it represents a trade-off that must be carefully weighed.
In clinical practice, ART is best reserved for cases in which conventional techniques have failed or are unlikely to succeed. It should not be viewed as a first-line treatment but rather as an advanced option for selected patients.
Complication Profile and Risk Management
The safety profile of ART is generally acceptable, but the procedure is associated with specific risks that require careful consideration. Graft displacement is one of the most common complications and can compromise surgical success. The use of perfluorocarbon liquids and appropriate tamponade agents can help stabilize the graft during and after surgery.
Retinal detachment, although relatively uncommon, is a serious complication that may occur due to extensive manipulation or preexisting retinal pathology. Prompt recognition and management are essential to preserve vision.
Epiretinal membrane formation represents another potential complication, likely related to glial proliferation. In some cases, this may necessitate additional surgical intervention.
Donor site complications, including localized scotomas, are an inherent aspect of the procedure. While these are typically asymptomatic, their potential impact should be discussed with patients during preoperative counseling.
Overall, meticulous surgical technique, careful patient selection, and thorough postoperative monitoring are critical to minimizing complications and optimizing outcomes.
Clinical Implications and Patient Selection
The introduction of ART has important implications for clinical practice. It expands the range of therapeutic options available to patients with refractory macular holes and offers hope in situations where traditional approaches have failed.
Patient selection is a key determinant of success. Ideal candidates for ART include individuals with:
- Large or chronic macular holes
- Previous unsuccessful surgical attempts
- Reasonable visual potential despite central damage
- Absence of severe comorbid retinal disease
Conversely, patients with advanced retinal degeneration, extensive atrophy, or poor overall ocular health may derive limited benefit from the procedure.
Preoperative counseling is essential to ensure that patients have realistic expectations. While anatomical closure is highly likely, visual improvement may be modest and gradual.
Technological Advances and Surgical Refinement
The success of ART is closely linked to advances in vitreoretinal surgical technology. High-resolution imaging, including optical coherence tomography (OCT), allows for precise assessment of macular anatomy and postoperative monitoring of graft integration.
Improvements in microsurgical instruments, including fine-gauge vitrectomy systems and specialized forceps, have enhanced the safety and precision of the procedure. The use of intraoperative OCT provides real-time feedback, enabling surgeons to optimize graft placement.
Future innovations may further refine the technique. Robotic-assisted surgery, for example, has the potential to improve accuracy and reduce variability in graft manipulation. Similarly, the development of novel tamponade agents and bioadhesives may enhance graft stability.
Future Directions and Research Opportunities
Despite its promise, ART remains an evolving technique with several unanswered questions. Future research should focus on:
- Standardization of Surgical Protocols: Variability in technique may influence outcomes. Establishing standardized guidelines could improve consistency and reproducibility.
- Long-Term Functional Outcomes: While anatomical success is well documented, long-term visual function requires further investigation.
- Biological Enhancement: Combining ART with regenerative therapies, such as stem cells or growth factors, may enhance graft survival and functional integration.
- Optimization of Graft Selection: Identifying the ideal size, location, and orientation of the graft could improve outcomes.
- Understanding Neural Integration: Research into synaptic connectivity and neural plasticity is essential for achieving true functional restoration.
Ethical and Practical Considerations
ART raises several ethical and practical considerations. The intentional creation of a retinal defect at the donor site represents a unique aspect of the procedure. While the functional impact is typically minimal, it underscores the importance of informed consent and careful patient selection.
Additionally, the technical complexity of ART may limit its availability to specialized centers with experienced vitreoretinal surgeons. Training and dissemination of expertise will be important for broader adoption.
Cost considerations may also play a role, particularly in resource-limited settings. The need for advanced equipment and extended surgical time may impact accessibility.
Conclusion
Autologous neurosensory retinal transplantation (ART) represents one of the most significant advancements in the surgical management of refractory macular holes and complex retinal pathologies in recent years. As vitreoretinal surgery continues to evolve, ART has emerged not merely as an alternative technique but as a transformative approach that addresses many of the fundamental limitations associated with conventional methods. By introducing viable, full-thickness autologous retinal tissue into the macular defect, ART shifts the paradigm from passive tissue approximation to active structural replacement and biological integration.
The clinical importance of this technique lies primarily in its ability to achieve consistently high anatomical closure rates in cases that have historically demonstrated poor prognosis. Refractory macular holes—particularly those that are large, chronic, or previously operated—pose a substantial challenge due to factors such as photoreceptor degeneration, retinal atrophy, and insufficient scaffolding for tissue repair. Traditional approaches, including repeat vitrectomy, internal limiting membrane peeling, and inverted flap techniques, often fail in these scenarios because they rely heavily on gliosis and limited regenerative capacity. ART overcomes these barriers by physically filling the defect with structurally robust tissue, thereby providing immediate mechanical stability and a platform for subsequent biological processes.
The evidence synthesized in this review indicates that ART achieves anatomical success rates exceeding 85–90% in refractory cases, a remarkable outcome considering the complexity of the patient population. Moreover, the durability of closure observed in long-term follow-up studies underscores the reliability of this technique. Once successful integration occurs, the likelihood of reopening appears minimal, suggesting that ART offers a stable and lasting solution for macular hole repair. This stability is particularly valuable in clinical practice, where repeated surgical interventions can increase both patient burden and risk of complications.
While anatomical success is a clear strength of ART, functional recovery remains a more nuanced outcome. Improvements in best-corrected visual acuity are generally modest but clinically meaningful. Many patients experience gradual gains in vision that enhance their ability to perform daily activities, even if full restoration of central visual acuity is not achieved. This discrepancy between anatomical and functional outcomes highlights the inherent complexity of retinal architecture, particularly in the foveal region, where precise photoreceptor alignment and synaptic connectivity are essential for high-resolution vision. In cases where long-standing disease has already caused irreversible damage, even the most successful structural repair cannot fully restore lost function.
Nevertheless, the functional improvements observed with ART should not be underestimated. Reduced metamorphopsia, improved retinal sensitivity, and better subjective visual quality contribute significantly to patient quality of life. These benefits are especially important in individuals who previously had limited or no viable treatment options. In this context, ART serves not only as a surgical intervention but also as a means of restoring functional independence and visual confidence.
A key aspect of ART’s success lies in its potential for biological integration. Postoperative imaging studies, particularly those utilizing optical coherence tomography, have demonstrated progressive incorporation of the graft into the host retina. In some cases, partial restoration of retinal layers and evidence of vascular integration have been observed, suggesting that the transplanted tissue is not merely a passive filler but an active participant in the healing process. The role of Müller cells, gliosis, and tissue remodeling appears central to this integration, although the exact mechanisms remain incompletely understood. Importantly, the extent to which synaptic connections are reestablished between the graft and host retina remains an open question and represents a critical area for future investigation.
Despite its advantages, ART is not without limitations. The procedure is technically demanding and requires a high level of surgical expertise, particularly in graft harvesting, manipulation, and positioning. The risk of complications such as graft displacement, retinal detachment, and epiretinal membrane formation necessitates meticulous technique and careful postoperative management. Additionally, the intentional creation of a donor site defect introduces an ethical and clinical consideration, even though these defects are typically located in the peripheral retina and are often asymptomatic.
Patient selection is therefore of paramount importance. ART is best suited for individuals with refractory macular holes who retain some degree of visual potential and do not have extensive retinal degeneration. Proper preoperative counseling is essential to ensure that patients have realistic expectations regarding outcomes, particularly with respect to the likelihood of partial rather than complete visual recovery. When applied in appropriately selected cases, ART offers a highly effective and meaningful therapeutic option.
Looking ahead, the future of ART is closely intertwined with advances in technology and regenerative medicine. Innovations such as intraoperative optical coherence tomography, refined microsurgical instruments, and robotic-assisted surgery have already enhanced the precision and safety of the procedure. Further developments in bioengineering, including the use of stem cells, growth factors, and bioadhesive materials, hold the potential to improve graft survival, integration, and functional outcomes. Additionally, a deeper understanding of neural plasticity and synaptic regeneration may pave the way for more complete restoration of visual function.
Standardization of surgical techniques and protocols will also be critical for broader adoption and reproducibility of results. As more clinical data become available, particularly from long-term and multicenter studies, a clearer consensus on best practices is likely to emerge. This will help reduce variability in outcomes and ensure that ART can be implemented more widely across different clinical settings.
From a broader perspective, ART exemplifies the ongoing shift in ophthalmology toward regenerative and restorative approaches. Rather than simply managing disease or preventing progression, modern surgical techniques increasingly aim to replace damaged tissue and restore function. In this regard, ART stands at the forefront of innovation, offering a glimpse into the future of retinal surgery.
In conclusion, autologous neurosensory retinal transplantation is a groundbreaking technique that has redefined the management of refractory macular holes and complex retinal diseases. Its ability to achieve high anatomical success rates, combined with meaningful functional improvements, makes it a valuable addition to the vitreoretinal surgeon’s armamentarium. Although challenges remain—particularly in achieving full functional restoration—the continued evolution of surgical methods and adjunctive therapies is likely to enhance outcomes further. As research progresses and experience grows, ART has the potential to become a cornerstone treatment for some of the most challenging conditions in retinal medicine, ultimately improving vision and quality of life for patients who previously had limited hope for recovery.
References
- Grewal DS, Mahmoud TH. Autologous neurosensory retinal free flap for closure of refractory myopic macular holes. JAMA Ophthalmol. 2016;134(2):229–230.
- Mahmoud TH, et al. Autologous retinal transplantation for macular hole: surgical technique and initial outcomes. Ophthalmology. 2017;124(10):1513–1518.
- Rossi T, et al. Autologous retinal transplant for recurrent macular holes: long-term outcomes. Retina. 2019;39(12):2319–2326.
- Caporossi T, et al. Autologous retinal transplantation for refractory macular holes: surgical technique and outcomes. Am J Ophthalmol. 2018;195:103–109.
- Grewal DS, et al. Functional and anatomical outcomes of autologous retinal transplantation for refractory macular holes. Retina. 2019;39(6):1139–1145.
- Morizane Y, et al. Autologous transplantation of the internal limiting membrane for refractory macular holes. Am J Ophthalmol. 2014;157(4):861–869.
- Michalewska Z, et al. Inverted internal limiting membrane flap technique for large macular holes. Ophthalmology. 2010;117(10):2018–2025.
- Chen SN, et al. Lens capsular flap transplantation in the management of refractory macular hole. Ophthalmology Retina. 2017;1(3):229–235.
- Rizzo S, et al. Autologous retinal transplantation for persistent macular holes: a pilot study. Graefes Arch Clin Exp Ophthalmol. 2018;256(9):1667–1674.
- Babu N, et al. Autologous retinal transplantation for refractory macular hole retinal detachment in high myopia. Retina. 2020;40(7):1325–1332.
- Grewal DS, Mahmoud TH. Autologous retinal transplant: current concepts and future perspectives. Curr Opin Ophthalmol. 2020;31(3):175–180.
- Steel DHW, Charles S. Vitrectomy fluidics in retinal surgery. Retina. 2011;31(8):1499–1508.
- Duker JS, et al. The International Vitreomacular Traction Study Group classification of macular holes. Ophthalmology. 2013;120(12):2611–2619.
- Ezra E. Idiopathic full-thickness macular hole: natural history and pathogenesis. Br J Ophthalmol. 2001;85(1):102–108.
- Christensen UC, et al. Value of internal limiting membrane peeling in macular hole surgery. Br J Ophthalmol. 2009;93(8):1005–1015.
- Shiode Y, et al. Autologous retinal transplantation for refractory macular holes: OCT-based analysis. Retina. 2021;41(6):1210–1217.
- Tanaka S, et al. Long-term outcomes of autologous retinal transplantation. Ophthalmology Retina. 2022;6(5):402–410.
- Frisina R, et al. Surgical outcomes and complications of autologous retinal grafting. Retina. 2020;40(11):2075–2083.
- Nawrocki J, et al. Autologous retinal free flap in macular hole surgery: indications and results. Acta Ophthalmol. 2020;98(5):e612–e618.
- Park JH, et al. Microperimetry outcomes after autologous retinal transplantation. Retina. 2021;41(9):1905–1912.